

Translate this page into:
Unmasking Mania: A case report of risperidone-induced mania in a schizophrenia patient

*Corresponding author: Shreya Batra, Department of Psychiatry, Government Medical College and Hospital, Chandigarh, India. sbbatra44@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Batra S, Bhattacharya S. Unmasking Mania: A case report of risperidone-induced mania in a schizophrenia patient. Arch Biol Psychiatry. 2024;2:81-3. doi: 10.25259/ABP_11_2024
Abstract
Risperidone is an atypical antipsychotic widely prescribed for the management of various psychiatric disorders, including schizophrenia. It is found to be most effective for treating the positive symptoms of psychosis and is also used for mania. Its mechanism of action is attributed to partial antagonism at serotonin and dopaminergic receptors. Through this mechanism, it has effectively treated the positive and negative symptoms of schizophrenia. However, there are few cases reported of risperidone-induced hypomania, a possible mechanism of this side effect is attributed to the partial agonistic action at the 5-HT2A receptors, by some authors. This case report presents the unique occurrence of manic symptoms due to risperidone in a 31-year-old male diagnosed with schizophrenia.
Keywords
Antipsychotics
Drug-induced mania
Mania
Psychotropics
Risperidone

INTRODUCTION
Second-generation antipsychotics are used for the treatment of manic symptoms. Still, there are few case reports in the literature of them causing dose-dependent manic symptoms such as elevated mood, over-talkativeness, and increased goal-directed activity as side effects. There is a review of case reports and series for all the antipsychotic-induced mania and hypomania out of which 22 cases were due to risperidone.[1] Of the many ways, they were treated, the most successful was changing the antipsychotic, stopping the current antipsychotic, or adding a mood stabilizer to the current antipsychotic regime; however, increasing the dose of the same antipsychotic was found unsuccessful.[1] There are case reports from India as well, where the patient was started on risperidone and they developed cheerful affect and were treated with adding mood stabilizer.[2] The following case report will shed light on the less discussed side effects of risperidone causing mania. Documenting such side effects is crucial for developing recommendations for dose adjustments, considering alternative therapies, and heightened caution in specific patient populations.
CASE REPORT
This is a case of, a 31-year-old male, Mr. MS, unmarried, unemployed, belonging to upper middle socioeconomic status residing in Chandigarh, India was admitted with a 4 years history of self-smiling, self-muttering, ideas of reference, and persecution, social and emotional withdrawal, decreased interaction with family members, verbal aggression with decreased appetite and subsequent weight loss with poor hygiene and significant socio-occupational decline.
The patient was, then, diagnosed with schizophrenia and started on T. risperidone 2 mg/d in 2019, his Brief Psychiatric Rating Scale (BPRS) (18 item) score decreased from 34 to 21. The patient was compliant with the treatment and maintained well on the same for 2 years, when a family member noticed hallucinatory behavior of the patient, at the time T. risperidone was increased to 3 mg/d. There were no affective symptoms at that time. His BPRS score was 28.
After 3 days of consumption of 3mg/d tablet, the patient reported feeling increased energy and reported it as equivalent to 10 red Bulls, irritability increased, got aggressive at family members, unlike his usual self, when, on follow-up, his risperidone was, further, increased to 4 mg/d, considering symptoms to be part of his illness. The next day patient would shout at the family members, pace in the room, felt decreased need for sleep, and would be found walking outside the house at odd times, felt increased energy, he also become overtalkative and it was difficult for the family members to stop him. Patient denies any substance use at the time and was compliant with risperidone.
The patient was then brought to our institute where T. risperidone was stopped as the emergence of symptoms had a temporal correlation with the up-titration of the dose of risperidone. Young mania rating scale (YMRS) score was 24. During the ward stay, the patient reported improvement in his symptoms and had normal sleep and appetite. T. olanzapine was started instead. After initiating T. olanzapine, the patient reported improvement in his symptoms and his YMRS score came down to 9 within 4 days of stopping T. risperidone. The association between the YMRS score and the doses of risperidone and olanzapine have been shown in Figure 1. The patient also reported subjective improvement with changing the antipsychotic/no hallucinatory behavior was observed during the ward stay and the patient was then discharged on T. olanzapine 10 mg/day. Naranjo adverse drug reaction scale was applied and the score came to be 5 which is a probable adverse drug reaction. The patient is currently on monthly follow-ups and is maintaining well on T. olanzapine 10 mg/day, and is compliant with the treatment. It is planned to shift the patient on antipsychotics with lesser propensity for switch such as lurasidone and aripiprazole. Written informed consent was obtained from the patient for publication of this report.
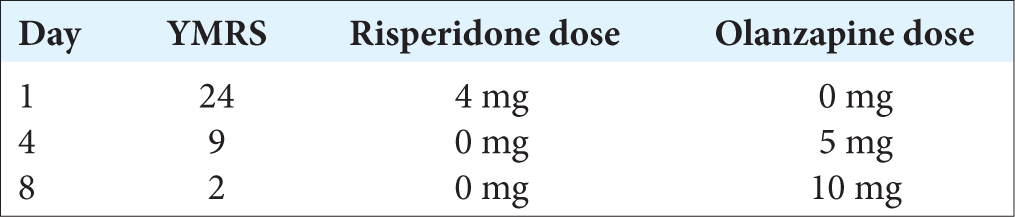
- Association between YMRS score and dose of risperidone and olanzapine.
DISCUSSION
There are approximately only two cases of risperidone-induced reported in India so far.[2] Some cases mentioned in the literature and the management done are shown in Table 1. In the index case, manic symptoms were observed within 2 days of increasing the dose of T. risperidone, with the YMRS of 24, after switching the tablet to T. olanzapine, the YMRS score decreased to 9 within 4 days suggesting a temporal correlation. No other mood stabilizer was required in the said case. The probable mechanism of the switch in the said patient can be the rapid increase in dose leading to rapid action at 5-HT2A receptors of risperidone. The resolution of symptoms with another antipsychotic can be due to compounding action on D2 receptors, and washout of risperidone action on 5-HT2A receptors. Few authors have mentioned these effects due to its action of partial agonism at 5-HT2A receptors, and also due to the dose-dependent effect of risperidone on 5-HT2A receptors and D2 receptors ratio.[3] Increased stimulation leads to increased prefrontal dopaminergic activity due to intrinsic 5-HT1A activation.[4] There may be some genetic predisposition for the development of manic switch in specific population groups.
| Author and Year | Clinical parameters | Diagnosis | Management |
|---|---|---|---|
| Dwight et al., 1994[4] | YMRS increased after risperidone | Schizoaffective disorder (six patients) |
Symptoms in a few patients resolved spontaneously on risperidone, and few had to be given valproate |
| Byerly et al., 1995[5] | Anxiety, restlessness, and insomnia after risperidone was titrated to 6 mg/d | Schizophrenia (four patients) | Self-limiting on risperidone 6 mg/d, some have to be given benzodiazepine cover |
| Tomlinson, 1996[6] | Euphoria and hypersexuality, pressured speech, and overfamiliarity when risperidone was titrated to 6 mg/d and haloperidol tapered to 10 mg/d | Schizophrenia (case report) | Risperidone was stopped and haloperidol increased to 80 mg/d, took 2 months to resolve |
| Barkin et al., 1997[7] | Two patients developed severe manic symptoms with risperidone titration | Schizophrenia (case series) | Cessation of risperidone, symptoms resolved spontaneously after 48 h |
| Zolezzi and Badr, 1999[8] | Manic symptoms of overspending, hypersexuality, and disinhibited behavior, 3 weeks after up-titrating dose of risperidone to 5 mg/d | Schizophrenia (four patients) | Risperidone was tapered and stopped; one patient showed improvement after 36 h. As symptoms did not resolve in some carbamazepine or chlorpromazine had to be added with benzodiazepine cover |
| Kavoor et al., 2014[2] | Manic symptoms such as overtalkativeness, grandiose ideas, irritability, increased psychomotor activity when risperidone was increased to 6 mg/d | Two patients 1: Schizophrenia 2: Acute transient psychotic disorder |
Risperidone was augmented with carbamazepine and lithium, respectively, there was improvement in affective symptoms. |
The studies have also suggested that change of antipsychotic have led to resolution of symptoms, some have also suggested it to be a paradoxical and self-limiting response to risperidone which did not require tapering of the dose, some required adding a mood stabilizer to existing regime, and some cases the dose of same antipsychotic were increased but no response with the same was seen. The time taken for remission was 36 h–2 months.[1]
CONCLUSION
This case highlights the importance of vigilance for paradoxical reactions, such as mania, especially during therapy initiation or adjustment. It contributes to the literature on antipsychotic-induced mood disturbances, underscoring the need for individualized patient monitoring and prompt intervention when adverse effects occur. Further studies are necessary to understand the underlying mechanisms and risk factors for such reactions. However, there are few limitations; this report is based on a single patient’s experience, which limits the generalizability of the findings. The occurrence of risperidone-induced mania may vary across different populations, and larger studies are needed to confirm this association. The possibility of other contributing factors that could influence the onset of mania independently of risperidone use cannot be ruled out.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Manic/hypomanic symptoms induced by atypical antipsychotics: A review of the reported cases. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30:549-64.
- [CrossRef] [Google Scholar]
- Risperidone-induced mania: An emergent complication of treatment. J Pharmacol Pharmacother. 2014;5:258-60.
- [CrossRef] [Google Scholar]
- The ratios of serotonin2 and dopamine2 affinities differentiate atypical and typical antipsychotic drugs. Psychopharmacol Bull. 1989;25:390-2.
- [Google Scholar]
- Antidepressant activity and mania associated with risperidone treatment of schizoaffective disorder. Lancet. 1994;344:554-5.
- [CrossRef] [Google Scholar]
- Behavioural stimulation associated with risperidone initiation. Am J Psychiatry. 1995;152:1096-7.
- [CrossRef] [Google Scholar]
- Induction of mania by risperidone resistant to mood stabilizers. J Clin Psychopharmacol. 1997;17:57-8.
- [CrossRef] [Google Scholar]




